How GLP-1 Hormones Are Rewiring Our Understanding of Chronic Disease
Originally developed for diabetes and weight loss, GLP-1 receptor agonists are now showing profound benefits for heart health, kidney function, and addiction.
By Factlen Editorial Team
- Systemic Health Researchers
- Medical professionals who view GLP-1s as a foundational treatment for metabolic syndrome.
- Addiction Neuroscientists
- Scientists exploring the off-label potential of GLP-1s to treat substance use disorders.
- Musculoskeletal Health Specialists
- Researchers concerned about the rapid loss of lean muscle mass during GLP-1 therapy.
- Editorial Synthesis
- Factlen's holistic view of the emerging science and its implications.
What's not represented
- · Insurance Providers
- · Patients experiencing severe GI side effects
Why this matters
GLP-1 medications are evolving from simple weight-loss tools into foundational treatments for the world's deadliest chronic diseases. Understanding their full systemic impact—and their risks—is crucial for anyone considering or currently managing their metabolic health.
Key points
- GLP-1 receptor agonists are demonstrating profound health benefits beyond weight loss, acting as systemic metabolic regulators.
- Recent massive clinical trials show the drugs reduce major cardiovascular events by 15% and composite kidney failure outcomes by 19%.
- The medications reduce vascular inflammation and stabilize arterial plaques independently of cholesterol or blood pressure changes.
- Receptors in the brain's reward centers allow GLP-1s to modulate dopamine, showing early promise in reducing cravings for alcohol and nicotine.
- Rapid weight loss on the medication can result in significant lean muscle loss, making resistance training a critical component of treatment.
- Discontinuing the medication typically leads to weight regain and the reversal of cardiometabolic benefits, suggesting a need for chronic administration.
For years, the narrative surrounding glucagon-like peptide-1 (GLP-1) receptor agonists like semaglutide and tirzepatide has been dominated by a single metric: the number on the scale. Originally developed to manage type 2 diabetes, these medications triggered a global phenomenon by enabling unprecedented, rapid weight loss.[8]
But as millions of patients have integrated these drugs into their daily lives, a far more profound medical story has begun to unfold. Clinical data is revealing that GLP-1 medications are not merely weight-loss tools; they are systemic metabolic regulators. From protecting the heart and preserving kidney function to potentially rewiring the brain's addiction pathways, these hormones are fundamentally reshaping our understanding of chronic disease.[8]
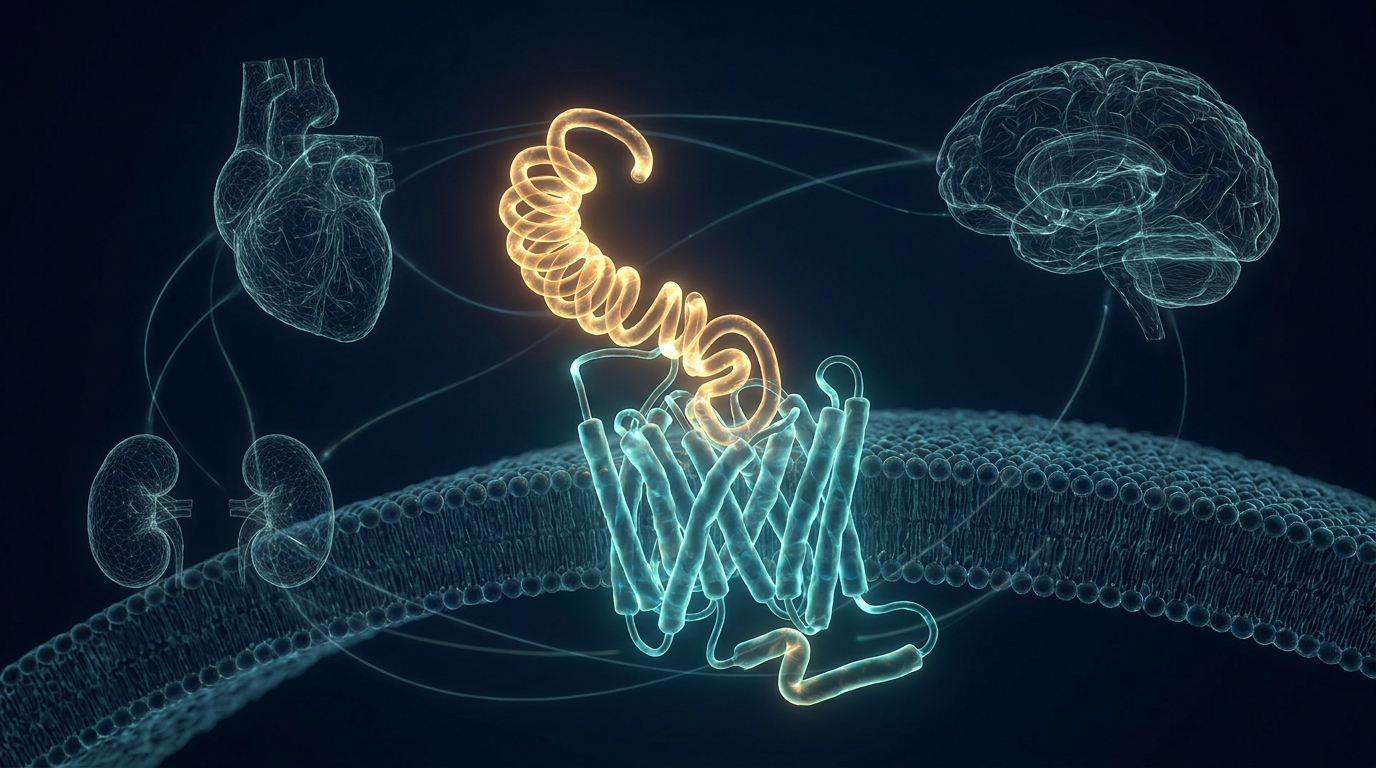
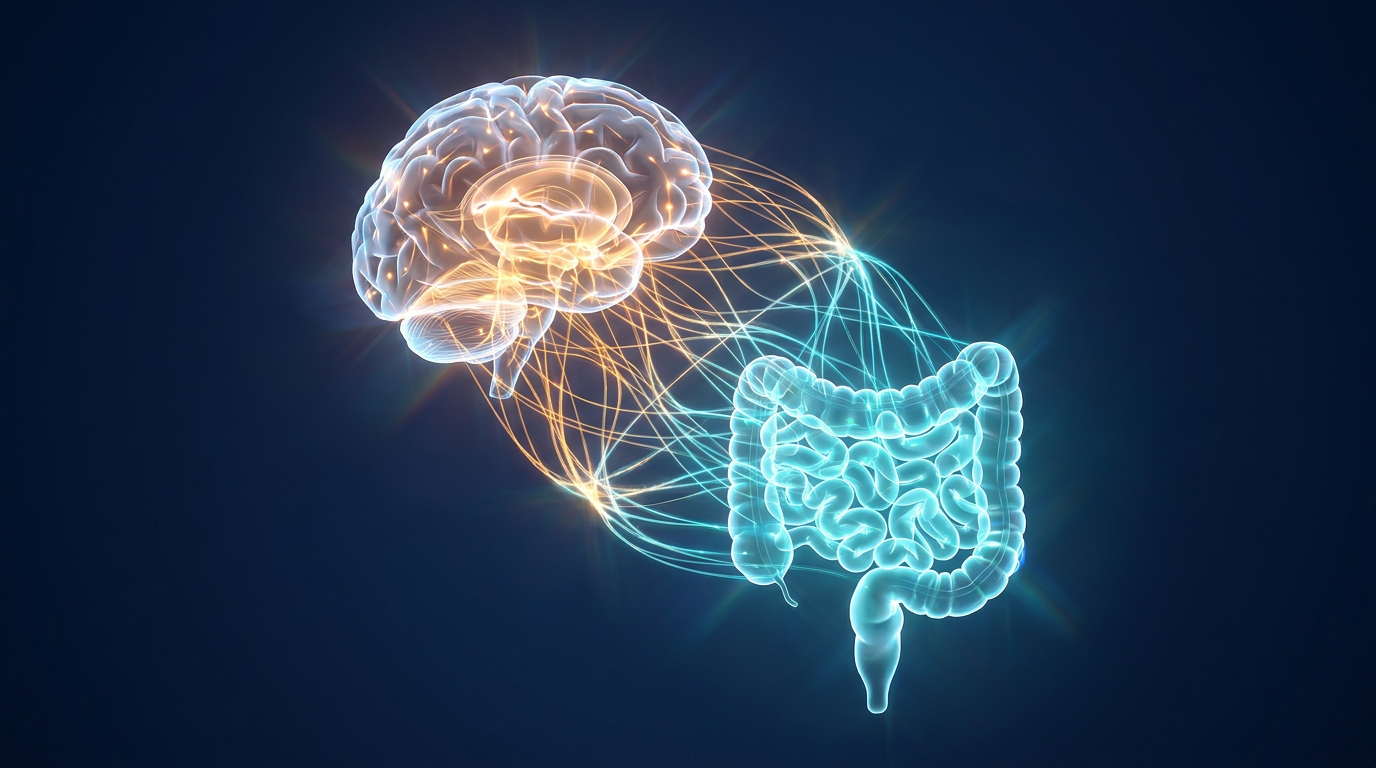
To understand how one molecule can affect so many different organs, it is necessary to look at the gut-brain axis. Natural GLP-1 is an incretin hormone secreted by the intestines in response to food. Its primary job is to prompt the pancreas to release insulin and block glucagon, keeping blood sugar stable after a meal.[2]
However, GLP-1 receptors are not confined to the pancreas. They are distributed widely throughout the human body, including in the heart, the kidneys, the vascular system, and the brain. By engineering synthetic versions of this hormone that last for days rather than minutes, scientists have inadvertently unlocked a master switch for systemic health.[2][5]

The most immediate and life-saving revelation has been in cardiovascular medicine. For decades, obesity has been treated as a primary driver of heart disease, with the assumption that losing weight would naturally ease the burden on the cardiovascular system. But recent outcome trials have shown that GLP-1 receptor agonists offer direct cardioprotective benefits that outpace what weight loss alone can explain.[2]
In major studies, patients taking these medications experienced a roughly 15 percent reduction in major adverse cardiovascular events, including heart attacks and strokes. Researchers have discovered that GLP-1 therapies improve endothelial function—the health of the inner lining of blood vessels—while simultaneously reducing oxidative stress and systemic inflammation.[2][6]
This anti-inflammatory effect is particularly crucial. Atherosclerosis, the dangerous buildup of plaque in the arteries, is driven heavily by inflammation. By stabilizing these plaques and reducing vascular inflammation independently of cholesterol or blood pressure changes, GLP-1 medications are acting as direct vascular protective agents. Furthermore, they have shown remarkable efficacy in treating heart failure with preserved ejection fraction (HFpEF), a notoriously difficult condition to manage.[2][5]
The protective halo extends downward to the kidneys. Chronic kidney disease (CKD) is a progressive, largely incurable condition that affects millions globally, often driven by diabetes and hypertension. For years, nephrologists have had limited pharmacological tools to halt its progression.[6]
A massive meta-analysis published in The Lancet Diabetes & Endocrinology, which pooled data from 19 clinical trials involving over 90,000 patients, confirmed a paradigm shift. The study found that GLP-1 receptor agonists reduced the risk of a composite renal outcome—including kidney failure and the need for dialysis—by 19 percent.[1][6]

The study found that GLP-1 receptor agonists reduced the risk of a composite renal outcome—including kidney failure and the need for dialysis—by 19 percent.
Crucially, these renal benefits were observed in patients both with and without diabetes. The medications appear to reduce microalbuminuria (protein leaking into the urine) by 24 percent, likely by lowering inflammation within the kidney tissues and improving how the organs handle sodium.[1]
Perhaps the most unexpected frontier for GLP-1 research lies inside the human brain. While the hormone's ability to signal fullness to the hypothalamus is well documented, scientists have recently mapped GLP-1 receptors in the ventral tegmental area (VTA) and the nucleus accumbens—the core architecture of the brain's reward and addiction circuitry.[3][7]
When a person consumes an addictive substance, whether it is alcohol, nicotine, or a highly palatable food, it triggers a surge of dopamine in these reward centers. Preclinical models and early human observations suggest that GLP-1 receptor agonists modulate this exact pathway. Rather than acting as a blunt dopamine blocker, the hormone appears to recalibrate the system, blunting the dopamine spike that drives compulsive craving.[3]
In animal models, GLP-1 therapies have successfully reduced the intake of alcohol, cocaine, and opioids, while also preventing relapse-like behaviors. Early-phase clinical trials in humans are currently investigating whether these metabolic drugs could become the next major pharmacological treatment for substance use disorders, offering hope for conditions that have historically seen limited pharmaceutical innovation.[3][7]

Despite these cascading benefits, the GLP-1 revolution carries significant uncertainties, chief among them being the composition of the weight lost. When patients shed 15 to 20 percent of their body mass rapidly, they are not just losing fat.[4]
Clinical studies indicate that between 25 and 40 percent of the weight lost on GLP-1 therapies comes from lean tissue, including skeletal muscle and bone density. In older adults, this rapid loss of lean mass can accelerate sarcopenia, leading to reduced physical strength, impaired mobility, and an increased risk of falls and fractures.[4]
Medical consensus is rapidly shifting to address this blind spot. Endocrinologists and obesity medicine specialists now emphasize that GLP-1 prescriptions must be paired with structured resistance training and high-protein diets. The goal is no longer simply maximizing weight loss, but optimizing the fat-to-muscle ratio to ensure long-term metabolic resilience.[4][8]

The second major challenge is the chronic nature of the treatment. Obesity and metabolic dysfunction are increasingly understood as chronic, relapsing conditions, much like hypertension. Data from extension trials demonstrate this starkly: when patients stop taking the medication, they frequently regain approximately two-thirds of their lost weight within a year.[8]
More concerningly, the cardiometabolic improvements—such as lowered blood pressure and improved cholesterol profiles—also revert toward baseline after the medication is withdrawn. This suggests that for many patients, GLP-1 therapy may need to be a lifelong commitment to sustain its systemic benefits.[8]
We are currently witnessing the adolescence of incretin-based medicine. What began as a targeted intervention for blood glucose has blossomed into a multi-system therapy that challenges the traditional boundaries between cardiology, nephrology, and psychiatry.[8]
As researchers continue to untangle the complex web of the gut-brain axis, the narrative of GLP-1 medications will continue to evolve. They are not a panacea, and their long-term effects on muscle mass and neurobiology require careful management. But by addressing the root metabolic dysfunctions that drive chronic disease, they offer one of the most significant leaps forward in preventative medicine in a generation.[8]
How we got here
2005
The FDA approves the first GLP-1 receptor agonist, exenatide, specifically for the management of type 2 diabetes.
2021
Semaglutide (Wegovy) receives FDA approval for chronic weight management after trials show unprecedented 15% body weight reductions.
2024
Cardiovascular outcome trials confirm that GLP-1 therapies directly reduce the risk of major heart events like strokes and heart attacks.
2025
A massive 19-trial meta-analysis reveals a 19% reduction in composite kidney outcomes, expanding the drugs' use into renal protection.
Viewpoints in depth
Systemic Health Advocates
Medical professionals who view GLP-1s as a foundational treatment for metabolic syndrome.
This camp argues that obesity and diabetes are merely symptoms of broader metabolic dysfunction. By targeting the GLP-1 pathway, they believe medicine can shift from treating individual symptoms—like high blood pressure or kidney decline—to addressing the root systemic cause. They point to the 15 to 20 percent reductions in major cardiovascular and renal events as proof that these drugs are essential preventative tools, advocating for broader insurance coverage and long-term, chronic administration.
Musculoskeletal Health Specialists
Researchers concerned about the rapid loss of lean muscle mass during GLP-1 therapy.
While acknowledging the metabolic benefits, these specialists warn of a looming crisis in body composition, particularly among older adults. They highlight that up to 40 percent of the weight lost on these medications is lean tissue and bone density. Their primary argument is that GLP-1 prescriptions are currently handed out without adequate lifestyle support, and they advocate for mandatory resistance training and protein monitoring to prevent drug-induced sarcopenia and frailty.
Addiction Neuroscientists
Scientists exploring the off-label potential of GLP-1s to treat substance use disorders.
This perspective focuses entirely on the brain. Because GLP-1 receptors are present in the ventral tegmental area and nucleus accumbens, these researchers see a novel mechanism for treating addiction. They argue that by modulating dopamine spikes rather than blocking them entirely, GLP-1 therapies could reduce cravings for alcohol, nicotine, and opioids without causing severe anhedonia (the inability to feel pleasure), representing a massive breakthrough for psychiatric medicine.
What we don't know
- Whether the reduction in addiction cravings seen in animal models will translate to long-term, FDA-approved treatments for human substance use disorders.
- The multi-decade effects of suppressing natural appetite and altering gut motility over a patient's entire lifespan.
- How to effectively transition patients off the medication without triggering rapid weight regain and the reversal of cardiovascular benefits.
Key terms
- GLP-1 Receptor Agonist
- A class of medications that mimic the natural incretin hormone GLP-1, stimulating insulin release, slowing digestion, and regulating appetite.
- Sarcopenia
- The age-related or rapid loss of skeletal muscle mass and strength, which can impair mobility and increase the risk of falls.
- Endothelial Function
- The health and performance of the inner lining of blood vessels, which plays a key role in regulating blood pressure and preventing clotting.
- Microalbuminuria
- An early sign of kidney damage characterized by abnormally high levels of a protein called albumin leaking into the urine.
- Ventral Tegmental Area (VTA)
- A region in the midbrain that is a primary component of the brain's reward circuitry, heavily involved in processing dopamine and addiction.
Frequently asked
Does GLP-1 medication only help with weight loss?
No. Recent clinical trials show GLP-1 therapies directly protect the heart and kidneys, and reduce vascular inflammation independently of weight loss.
Can these drugs treat addiction?
Early research suggests they can. GLP-1 receptors in the brain's reward centers help modulate dopamine, which has been shown to reduce cravings for alcohol and nicotine in preclinical models.
What happens to muscle mass on GLP-1s?
Studies indicate that 25 to 40 percent of the weight lost can be lean tissue, including muscle. Doctors strongly recommend pairing the medication with resistance training and a high-protein diet.
Do the health benefits last if you stop taking the medication?
Typically, no. Trials show that patients regain a significant portion of the weight and lose the cardiovascular improvements within a year of stopping the drug.
Sources
Source coverage
8 outlets
4 viewpoints surfaced








[1]The Lancet Diabetes & EndocrinologySystemic Health Researchers
Effects of GLP-1 receptor agonists on kidney and cardiovascular disease outcomes: a meta-analysis of randomised controlled trials
Read on The Lancet Diabetes & Endocrinology →[2]Journal of Clinical InvestigationSystemic Health Researchers
Cardiovascular benefits of GLP-1 receptor agonists
Read on Journal of Clinical Investigation →[3]Medical SciencesAddiction Neuroscientists
Mechanisms of GLP-1 in Modulating Craving and Addiction: Neurobiological and Translational Insights
Read on Medical Sciences →[4]Frontiers in EndocrinologyMusculoskeletal Health Specialists
Musculoskeletal consequences of GLP-1 therapy in older adults
Read on Frontiers in Endocrinology →[5]Cardiac Failure ReviewSystemic Health Researchers
GLP-1RAs in Heart Failure: Beyond Glycaemic Control
Read on Cardiac Failure Review →[6]American Journal of Kidney DiseasesSystemic Health Researchers
Kidney and cardiovascular outcomes among patients with CKD receiving GLP-1 receptor agonists
Read on American Journal of Kidney Diseases →[7]National Institutes of HealthAddiction Neuroscientists
Glucagon-like peptide-1 receptor agonists and substance use disorders
Read on National Institutes of Health →[8]Factlen Editorial TeamEditorial Synthesis
Synthesis by Factlen editorial team
Read on Factlen Editorial Team →
More in health
See all 5 stories →Longevity Science
The Ultimate Longevity Metric: Why VO2 Max Outperforms Traditional Health Markers
8 sources

Metabolic Health
How a 20-Year Study Proves Simple Lifestyle Changes Prevent Chronic Disease
7 sources

Mitochondrial Health
The Science of Zone 2 Training: How Moderate Exercise Extends Healthspan
7 sources

Every angle. Every day.
Get health stories with full source coverage and perspective breakdowns delivered to your inbox.