Wearable Data Reveals GLP-1 Weight Loss Paradox: Users Significantly Decrease Daily Physical Activity
A new study analyzing Fitbit data from 753 patients reveals that adults taking GLP-1 weight-loss medications move significantly less after starting treatment. The findings highlight the critical need for mandatory exercise to prevent severe muscle loss during rapid weight reduction.
By Factlen Editorial Team

- Clinical Endocrinologists
- Argues that the metabolic risk of muscle loss makes exercise a mandatory co-prescription with GLP-1s.
- Behavioral Health Experts
- Emphasizes that severe calorie deficits naturally induce fatigue and reduce spontaneous movement.
- Fitness & Rehabilitation Professionals
- Advocates for resistance training as the primary mechanical intervention to preserve lean mass during weight loss.
What's not represented
- · Patients who successfully maintained muscle mass on GLP-1s
- · Wearable technology manufacturers
Why this matters
GLP-1 medications cause patients to lose significant amounts of lean muscle mass alongside fat. If users naturally decrease their physical activity while on the drug, they accelerate this muscle loss, leading to a weaker metabolism and a higher risk of rapid weight regain once the medication is stopped.
Key points
- Wearable data from 753 patients shows daily steps drop by an average of 560 after starting GLP-1 medications.
- Moderate-to-vigorous physical activity also fell from 28 to 22 minutes per day.
- The steepest declines in movement were observed in men and individuals with pre-existing musculoskeletal pain.
- Because GLP-1s reduce lean muscle mass alongside fat, a decrease in physical activity accelerates muscle wasting.
- Medical professionals emphasize that resistance training must be a mandatory co-prescription with GLP-1 therapy.
The medical community has long operated on a logical assumption regarding weight loss: as people shed pounds, moving becomes physically easier, joints bear less mechanical load, and spontaneous physical activity naturally increases. The advent of highly effective glucagon-like peptide-1 (GLP-1) receptor agonists like semaglutide and tirzepatide seemed poised to trigger a wave of newfound mobility. However, objective wearable data has unmasked a behavioral paradox. Rather than moving more, patients utilizing these medications experience a significant, measurable decline in their daily physical activity.[1][3]
The findings, presented at the Endocrine Society’s ENDO 2026 annual meeting in Chicago, dismantle the expectation of automatic activity increases. Researchers from HSHS St. John’s Hospital analyzed data from 753 adults with obesity who had been prescribed a GLP-1 medication. By utilizing the National Institutes of Health’s All of Us Research Program, the team linked electronic health records directly to continuous Fitbit activity data. This methodology bypassed the notoriously unreliable nature of self-reported exercise journals, providing an unvarnished look at how human behavior shifts when pharmaceutical appetite suppression takes hold.[3][4][5][6]
The objective data revealed a stark downward trend. Following the initiation of GLP-1 therapy, the cohort’s average daily step count dropped from 5,047 to 4,487—a statistically significant decrease of 560 steps per day. Furthermore, the time spent in moderate-to-vigorous physical activity (MVPA) fell from roughly 28 minutes to 22 minutes daily. The expected rebound in movement simply did not materialize in the data; instead, the medication induced a state of physical conservation.[2][3][4][7]

The decline was not distributed evenly across the population. The steepest reductions in movement were isolated among male participants, who recorded an average drop of 986 steps per day compared to a 445-step decline in women. Individuals suffering from pre-existing musculoskeletal pain also exhibited disproportionately large drops in activity. Conversely, variables such as chronological age, chronic heart failure, or a history of stroke did not alter the overarching downward trajectory, suggesting the lethargy is a broad physiological response to the treatment rather than a niche side effect.[2][4][5][8]
Understanding this paradox requires examining the physiological reality of rapid, medically induced calorie deficits. When a GLP-1 medication effectively suppresses appetite, the body enters a severe energy shortfall. The natural biological response to a sudden drop in caloric intake is the down-regulation of non-exercise activity thermogenesis (NEAT)—the subconscious movements, fidgeting, and casual walking that make up daily activity. Patients simply have less available energy, making exercise feel significantly more taxing.[2][7]
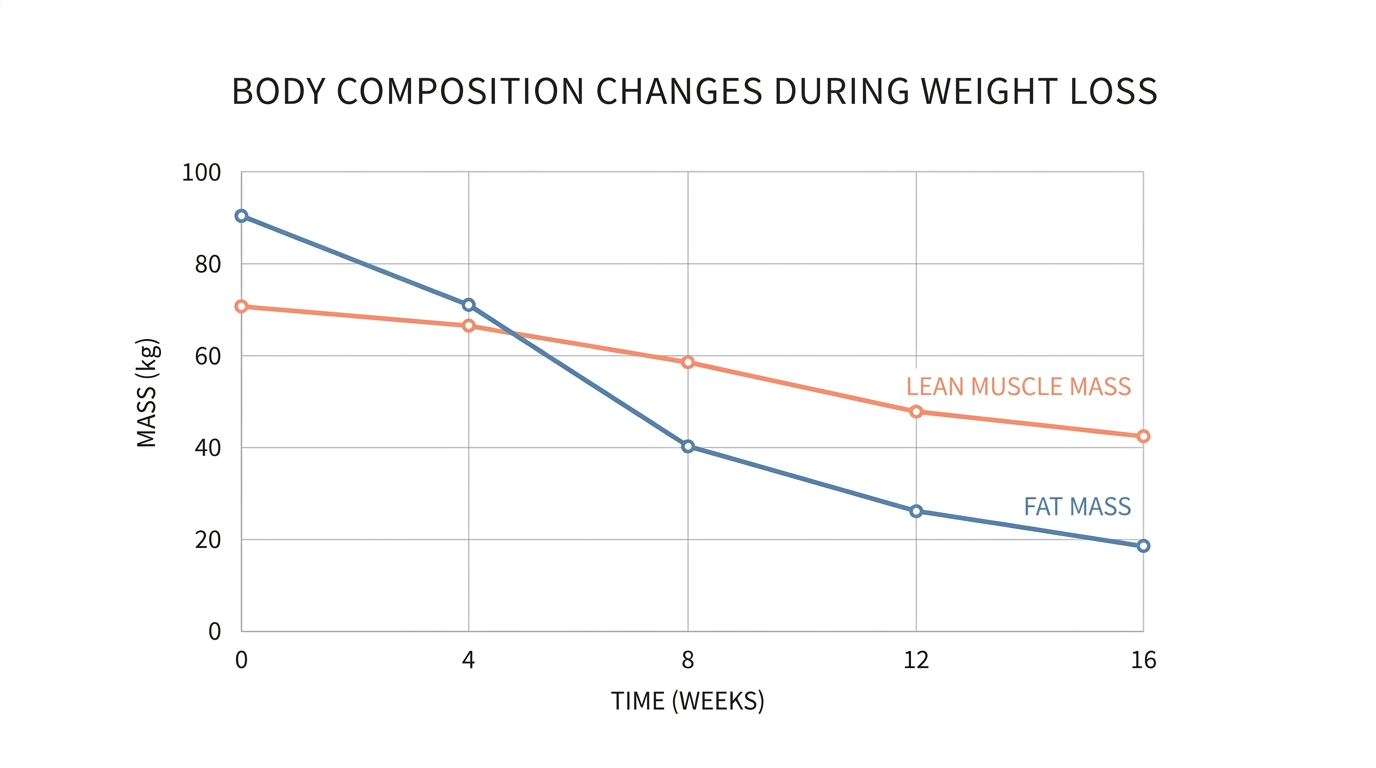
This decline in movement creates a severe clinical threat because of how GLP-1 medications alter body composition. These drugs do not selectively target adipose tissue; they reduce overall body mass. Multiple clinical analyses have documented that between 25 percent and 40 percent of the total weight lost on GLP-1 therapies consists of lean mass, including vital skeletal muscle and connective tissue.[5][7]
This decline in movement creates a severe clinical threat because of how GLP-1 medications alter body composition.
The compounding nature of this problem is what alarms endocrinologists. The medications actively strip away muscle tissue, while the simultaneous reduction in daily physical activity removes the primary mechanical stimulus that would otherwise signal the body to preserve that muscle. Reducing lean mass while dropping scale weight mathematically lowers body fat percentage, but it leaves the patient with a weaker metabolic engine, increased physical fragility, and a highly compromised baseline for long-term health.[5][6][7]
In a side-by-side trade-off analysis, the medical community is now evaluating two distinct approaches to GLP-1 therapy. The first is the 'Passive Weight Loss Model,' where patients rely entirely on the medication's appetite suppression without structured exercise interventions. The primary evidence for this approach is its exceptionally high initial compliance rate; it requires minimal behavioral friction and delivers rapid, effortless reductions in total scale weight.[2][7]
However, the evidence against the passive model is mounting. By allowing lean muscle to waste away alongside fat, the passive approach significantly lowers the patient's basal metabolic rate. When the metabolic engine shrinks, the body requires fewer calories to survive. If the patient ever discontinues the medication, this lowered metabolic rate creates a prime environment for rapid, disproportionate fat regain—a phenomenon that leaves the individual with a worse body composition than before they started treatment.[2][5][7]
Conversely, the 'Active Preservation Model' mandates the pairing of GLP-1 medications with structured, moderate-to-vigorous physical activity, specifically prioritizing resistance training. The evidence for this approach centers on mechanical tension. When muscles are subjected to the stress of lifting weights or resistance bands, it signals the central nervous system to spare muscle tissue during a caloric deficit, forcing the body to prioritize fat stores for energy instead.[6][7]

The evidence against the active model lies entirely in behavioral friction. It requires patients to actively fight against the drug-induced fatigue and the lethargy of a calorie deficit. Furthermore, because muscle tissue is dense, patients adhering to the active model may see their total scale weight drop more slowly, which can be psychologically discouraging despite being physiologically superior.[2][5][7]
Evaluating these trade-offs requires clear clinical guidance. The passive, medication-only approach fits well only in acute scenarios where severe obesity poses an immediate, life-threatening cardiovascular risk, and where physical movement is strictly medically contraindicated. In these rare cases, rapid total mass reduction takes absolute precedence over muscle preservation.[4][7]
In contrast, the active preservation approach fits well for the vast majority of patients seeking long-term metabolic healthspan. It is the only viable model for preventing sarcopenic obesity—the dangerous combination of low muscle mass and high body fat—and for ensuring that the weight lost results in a stronger, more capable physical frame rather than a fragile one.[5][6]

The data from the ENDO 2026 presentation serves as a definitive wake-up call for both prescribers and patients. The assumption that the drug will 'do all the work' is not just inaccurate; it is physiologically hazardous. As lead researcher Dr. Sajana Maharjan explicitly noted, the findings reinforce that exercise cannot be viewed as an optional accessory for people taking these medications. It must be treated as a mandatory, co-prescribed intervention to protect the body's structural integrity while the medication manages the metabolic load.[2][3][4][6][7]
How we got here
2021–2023
GLP-1 medications like Wegovy and Zepbound gain widespread approval and popularity for obesity treatment.
Early 2024
Clinical reports begin highlighting the significant loss of lean muscle mass alongside fat in GLP-1 patients.
June 14, 2026
Researchers present the Fitbit wearable data study at the ENDO 2026 conference, proving a measurable decline in physical activity among users.
Viewpoints in depth
Clinical Endocrinologists
Focuses on the metabolic risks of muscle wasting and the necessity of prescribing exercise.
Medical professionals emphasize that GLP-1 medications are not a standalone cure for obesity. Because these drugs strip away lean muscle mass alongside fat, endocrinologists warn that a passive approach to weight loss leaves patients physically fragile. They argue that exercise must be treated as a mandatory co-prescription to protect the patient's long-term metabolic health and prevent rapid weight regain if the medication is ever discontinued.
Behavioral Health Experts
Focuses on the physiological fatigue and calorie-deficit lethargy that naturally reduces spontaneous movement.
Behavioral researchers point out that the decline in physical activity is a natural physiological response to a severe energy deficit. When GLP-1s suppress appetite, the body instinctively down-regulates non-exercise activity thermogenesis (NEAT) to conserve energy. This camp argues that patients are not simply 'slacking off'; they are battling drug-induced fatigue and require targeted behavioral interventions to overcome the lethargy.
Fitness & Rehabilitation Professionals
Focuses on resistance training as the primary mechanical intervention to save lean mass.
The fitness community views the GLP-1 activity paradox as a mechanical problem with a mechanical solution. They argue that cardiovascular exercise alone is insufficient to prevent muscle wasting during rapid weight loss. Instead, they advocate for heavy resistance training, which provides the necessary mechanical tension to signal the central nervous system to preserve muscle tissue, forcing the body to burn fat stores instead.
What we don't know
- Whether the decline in physical activity persists long-term or if patients eventually adapt to the calorie deficit and resume movement.
- Exactly how much resistance training is required to fully offset the muscle-wasting effects of GLP-1 medications.
Key terms
- GLP-1 Receptor Agonist
- A class of medications that mimic a natural hormone to regulate blood sugar, slow digestion, and significantly reduce appetite.
- Moderate-to-Vigorous Physical Activity (MVPA)
- Activities that raise the heart rate and induce sweating, ranging from brisk walking to heavy weightlifting.
- Lean Muscle Mass
- The total weight of the body's muscle tissue, crucial for maintaining metabolic rate, physical strength, and bone density.
- Basal Metabolic Rate (BMR)
- The number of calories the body burns at rest to maintain basic life-sustaining functions.
- Sarcopenic Obesity
- A condition characterized by the simultaneous presence of excess body fat and dangerously low muscle mass or strength.
Frequently asked
Do GLP-1 medications directly cause fatigue?
While the drugs can cause some fatigue as a side effect, the primary driver of reduced energy is the significant calorie deficit created by the medication's appetite-suppressing effects.
How much muscle do people typically lose on GLP-1s?
Clinical studies indicate that between 25% and 40% of the total weight lost on medications like semaglutide and tirzepatide can be lean mass, including muscle and bone density.
What type of exercise is best for GLP-1 users?
Resistance training, such as weightlifting or bodyweight exercises, is considered the most critical form of exercise to signal the body to preserve muscle tissue during rapid weight loss.
Did the study rely on patients remembering their exercise?
No, the ENDO 2026 study was unique because it used objective, continuous data from Fitbit wearable devices linked to electronic health records, eliminating self-reporting bias.
Sources
Source coverage
8 outlets
3 viewpoints surfaced








[1]HealthlineFitness & Rehabilitation Professionals
People Using GLP-1s, Like Ozempic, Wegovy, Less Likely to Exercise Despite Benefits
Read on Healthline →[2]Global NewsBehavioral Health Experts
GLP-1 users decrease daily physical activity
Read on Global News →[3]Endocrine SocietyClinical Endocrinologists
Exercise decreases among people taking GLP-1 medication
Read on Endocrine Society →[4]HealioClinical Endocrinologists
Patients with obesity exercise less after starting GLP-1s
Read on Healio →[5]Neuroscience NewsBehavioral Health Experts
GLP-1 Weight Loss Paradox: Users Move Less, Risking Muscle Mass
Read on Neuroscience News →[6]Contemporary HealthClinical Endocrinologists
A counterintuitive picture of how people move on GLP-1s
Read on Contemporary Health →[7]Roid AppFitness & Rehabilitation Professionals
The GLP-1 Activity Paradox: Why Users Are Moving Less
Read on Roid App →[8]Drugs.comFitness & Rehabilitation Professionals
People Walk, Exercise Less After Starting Ozempic, Zepbound
Read on Drugs.com →

Every angle. Every day.
Get fitness stories with full source coverage and perspective breakdowns delivered to your inbox.